
The aim of this website is to provide information about the Tarlov Cyst disease and it is designed for educational and informational purposes. Here you will find news and personal experiences about this medical condition.
Tarlov cysts, also known as perineurial cysts or sacral nerve root cysts. They are named for neurologist Isadore M. Tarlov, who described them in 1938.
They are dilations of the nerve root sheaths and are abnormal sacs filled with cerebrospinal fluid (hereafter referred to as CSF) that can cause a progressively painful radiculopathy (nerve pain). The fluid in the cyst can put pressure on the nerve inside and on the adjacent nerve roots and cause debilitating symptoms.
Tarlov cysts differ in structure, they might incorporate nerve elements or be free of them. A cyst can be valved or non-
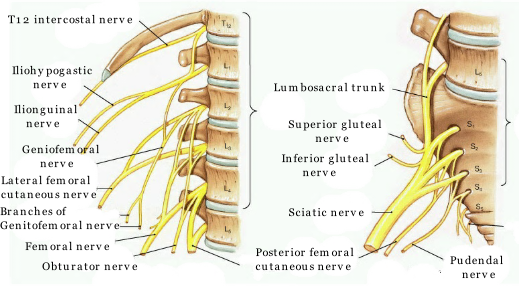
They are located most prevalently in spinal canal of S1 to S4 region of vertebrae and can be distinguished from other meningeal cysts by nerve-
The cyst is the nerve and therefore cannot be cut out.
These cysts are often detected incidentally during MRI, CT and Myelogram scans for other medical conditions. Tarlov Cysts are relatively common when compared to other neurological cysts.. Although originally believed by Tarlov to be asymptomatic lesions, these cysts, when present in the sacral neural canal and foramina, have since been found to cause a variety of symptoms.
The annual incidence of perineural cysts is estimated at approximately 5%, although large cysts that cause symptoms are relatively rare with annual incidence estimated at less than 1/2,000. Women are affected more frequently than men.
Causes of Tarlov Cyst
The cause of these cysts is still unknown, there are several hypotheses proposed regarding the formation of Tarlov Cysts, including: inflammation within the nerve root cysts followed by inoculation of fluids (epidurals), developmental or congenital origin, trauma. Some incidents or conditions that might potentially cause the asymptomatic cysts to become symptomatic are traumatic injuries such as falls, automobile accidents , heavy lifting, childbirth. Trauma to the spinal cord, an increase in the CSF pressure, or a blockage of the CSF can result in cyst formation.
Symptoms
Symptoms can vary depending on the location of the cysts, size and the section of the spine they occur:
- Pain with sitting. May feel like you are sitting on a rock or an object.
- Pain with standing
- Pain or numbness in the buttocks or between the legs
- Leg weakness or numbness
- Pulling and burning sensation in coccyx (tailbone) area, especially when bending
- Pain in the legs and feet especially in the back of the thighs
- Pain in the chest, upper back, neck, arms and hands
- Pain with sexual intercourse
- Inability to empty the bladder or in extreme cases to urinate at all
- Bowel or bladder changes, including incontinence
- Headaches and sometimes accompanied by blurred vision, double vision, pressure behind the eyes and optic nerve pressure causing papilledema (optic nerve swelling)
- Dizziness and feeling of loss of balance or equilibrium, especially with change of position
- Vaginal, rectal, pelvic and/or abdominal pain
Diagnosis and treatment
Effective examination method for Tarlov Cysts are MRI and CT. Both of them are good imaging procedures that allow the detection of extradural spinal masses such as Tarlov cysts. The best imaging study to image the Tarlov/perineural cyst is a spine MRI, and since the vast majority of the perineural cysts are on the sacral spine, then the order should be for a "full sacral spine MRI (S1-
A CT with Myelography is diagnostic tool that uses radiographic contrast media (dye) that is injected into the spinal canal’s fluid (cerebrospinal fluid, CSF). After the dye is injected, the contrast dye serves to illuminate the spinal canal, cord, and nerve roots during imaging. Thus, when a CT scan and myleography are combined, images are produced that clearly show both the bony structures of the spine and the nerve structures. These images are invaluable to physicians as they diagnose a patient’s spine problem.
When faced with a patient asking about a MRI report that indicate a possible Tarlov Cyst , the specialist may consult a neuroscience textbook and find there the initial mistaken supposition of Mr Tarlov that these cysts would not cause pain. This notion was contradicted by clinical experience and corrected in journal articles by Tarlov and others, but misinformation on this aspect of Tarlov Cysts persist in medical books and this result in denial of pain management, disability status and treatment. Untold numbers of persons with this disease suffer for long period without diagnosis or treatment.
Despite advancements in diagnosis, there remains a great deal of controversy regarding the optimal treatment of symptomatic Tarlov Cysts. There are some treatments available for alleviating the symptoms caused by these cysts. Their effectiveness is “personal”. Every case is different, it depends of number of cysts, size, location, age of the patient and more.
There is not compelling evidence that chiropractic, physical therapy or any other conservative manual or physical treatment is effective in treating symptomatic TC’s.
Non-
Pain may be temporarily controlled by aspiration of the cysts and then injecting the cysts with fibrin glue (a substance produced from blood chemicals involved in the clotting mechanism). The aspiration of CSF and injection of fibrin glue procedure theoretically is designed to remove the CSF from the cyst, and to block the entrance or the neck of the cyst with the sealant glue, to prevent return of the flow of CSF into the cyst. Some patients have found immediate relief after the procedure, while others have reported a delayed benefit from the procedure when the nerve irritation has subsided. After the procedure, there are outcomes of both short term relief, as well as longer term relief reported. However, it is considered to be a temporary relief procedure.
Surgery may be the treatment of choice when the pain is intractable, the sacrum is eroding and remodeling and the neurological symptoms become severe. Before referring to a spine surgeon, find out in advance if the surgeon dismisses TC’s as asymptomatic or not surgically treatable. This could save you, time, money and aggravation. There are a small number of physician's in the world who have surgical expertise in the treatment for TCs, and the short-
The usual surgical procedure consists of fenestration and imbrication of the cysts and then packing all the dead space around the cysts with fat, glue, and/or muscle. The body does not like dead spaces, and new cysts will possibly develop in the dead spaces around the old cysts, if not filled. Due to the potential risks for further nerve damage or spinal fluid leaks, there might be increased symptoms postoperatively, including more bowel and bladder problems, when the cysts are located in the S2-
For more detailed information, please visit the Tarlov Cyst Disease Foundation.
Treatment in UK and abroad
There are few surgeons in the world that can operate a Tarlov Cyst. The world’s specialist is Dr Feigenbuan from Dallas, Texas, USA.
Dr. Feigenbaum's practice routinely treats patients with giant meningeal cysts from all over the United States and other countries(Cyprus).
DR Casey from London uses a similar technique to Dr Feigenbuam and that this is available in the UK.
Dr. Dorte Clemmensen is available in Denmark for treatments.
The treatment is not available under the NHS, either routinely or through specialised commissioning and they do not routinely commission the treatment because of a lack of evidence for its effectiveness. The NHS’s responsible commissioner.
This is the reason Ms Beathrice Viviani, from Bournemouth, was given when her application for a state founded treatment in another European Economic Area (S2),was rejected by the Border Healthcare Team (NHS England) after travelling to Cyprus to have her Tarlov Cyst treated privately by Dr Feigenbaum at the AIMIS Spine Centre.
Ms Viviani had to use all her savings (£30.000) to pay for the surgery that saved her from being bed ridden and on a wheel chair for the rest of her live.
Contacts:
- Dr Frank Feigenbaum, USA: http://frankfeigenbaum.com/
- AIMIS Spine Cyprus -
Tarlov Cyst: https://www.aimisspine.com/condition/tarlov-meningeal- cysts/ - Dr Dorte Clemmensen in Denmark:
http://www.neurokirurgen.dk/tarlov-
Useful links:
Tarlov Cyst Disease Foundation
What is tarlov cyst?



Multiple Tarlov Cysts






Tarlov Cyst
“Sitting was unbearable without a cushion... daily life became a struggle”
Follow us: @MailOnline on Twitter | DailyMail on Facebook






Thank you for visiting this page, take care. Beathrice end Roberto

Tarlov Cyst Disease UK
Please help us to keep this web site running